Riders For Health is an NGO set up by Barry and Andrea Coleman alongside Randy Momola in 1996. The scheme trains mobilizes health workers in order to reach rural areas and cater for the healthcare needs. They do various things such as HIV testing to health education sessions. The healthcare workers are mobilized by motorbikes in which they are trained in maintaining therefore they can reach rural ares over tough terrain. R4H is in seven different African countries and was introduced into Kenya in 2002.
Kenya and R4H (brief of AIB)
(Page 3) Kenya's health profile looks like this
- Population - 45 million
- Life expectancy - 63 - up 3 in 4 years
- IMR - 40.71/1000 - halved in 4 years
- Maternal Mortality rate - 3.6/1000
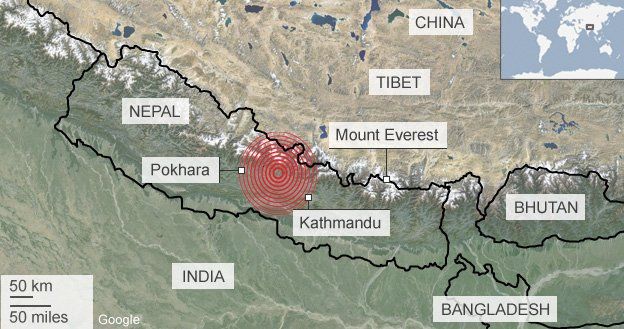
(Page 4) R4H was set up as mentioned by Andrea, Barry and Randy. They registered that many bikes were being left unattended and not working due to simple problems such as a flat tyre. They saw the opportunity that if they could fix them up and get them running then more healthcare would be delivered especially in tough terrain rural area that 60% of Kenya live on. R4H was announced n NGO in 1996 and operate in 7 countries across Africa.
(Page 5) They began operations in 2002 and they have 8 staff who manage 77 vehicles. The R4H bases are in Kisumu (western) and Nairobi (central).
(Page 6) In 2011 a training academy was set up in order to help riders develop skills such as driving, maintaining and journey planning with their bikes. An extra 20,000 people across Kenya can be reached due to the R4H. This is mainly due to travel time being cut from 4 hours down to 1. and being able to reach 80KM away instead of only 20KM.
(Page 7) The terrain and relief in Kenya is very varied. The highest areas are in the south western areas on the borders with Uganda and Tanzania. Kisumu where the academy was set up is located here and has relief of over 1000m.
(Page 8) Precipitation is also highest in these south western areas, with places such as Kisumu getting 2000mm+ of rainfall a year. This coincides with the higher the land the more rain which makes the terrain more difficult.
(Page 9) Cropland is once again highest in southwestern area such as Kisumu, this could be due to the relief and weather. Agriculture and crops is the main contributor to the nations GDP. Therefore there will be many rural communities that require healthcare. If better healthcare, better productivity.
(Page 10) Once again the southwestern rural areas have the highest population density with 600+ people per square KM in Kisumu. The main trend of the south western areas are between 100-599 people per square km. These people will therefore need healthcare.
(Page 11) Once again this coincides with the density of poverty which is in this region is high, Kisumu has 200+ people living on less that $2 a day per square km. This has a direct correlation with the healthcare needed in these areas and why bikes are so important.
(Page 12) There are many issues in Kenya regarding logistics of healthcare. The goods are supplied by KEMSA who are not very efficient and don't meet the needs of the people. The supplies are taken from Mombasa (coast) to central Nairobi and then to outlying warehouses. However there is a problem when it comes to the amount distributed to each area, the amount is based on the proportion of population living there and not to the areas that need it most. The deliveries are by lorries that struggle with rough terrain. The poor communications infrastructure gives local people no chance of ordering supplies according to local needs. The poor transport infrastructure makes it slow and unreliable to whether the supplies will reach the needed places. To improve an IT system needs to be put in place which will adapt the system to who needs it most. The delivery f the drugs could also be improved by vehicles better suited to rough terrain (motorbikes or 4x4).
Spending in the government is currently focusing on increasing the numbers of healthcare professionals and not on improving the infrastructure. I think this is a problem as many of the workers are moving to better paid posts abroad, and therefore the government are spending on the symptom and not the cause. There is a clear shortage of trained staff nationally but especially in rural areas where the number of patients to doctors is much lower than in urban areas.
(Page 13) There is an idea called rotating expat program which is to attract and develop talent from across the globe to come to Kenya to practice and train others in medicine for up to 2 years. This would benefit both countries. This would increase the numbers of workers and hopefully with a similar programme move some of the workers from urban to rural areas.
(Page 14) Millenium development goals are 8 goals set in 2000 to be achieved by 2015.
- eradicate hunger and poverty
- universal primary education
- gender eequality
- reduce IMR
- improve maternal health
- combat HIV/Aids and other diseases
- ensure environmental sustainability
- develop global partnership
In 2005 it was said that the country were unlikely to achieve any of the MDGs due to lack of resources. A plan was put in place to help achieve the goals and one of the sections was 'strengthening service delivery systems'. This clearly relates to R4H. It is clear that investment works best when it is within a clearly structured health service with long term priorities. The main components of a functioning health system includes:
- human resources
- infrastructure
- management capacity
Kenya has 500 hospitals, 611 health centres and 3310 sub centres. Each hospital has a raatio of 1:60000 people. Only 25% of Kenyans had access to health facility within 8KM.
Health expenditure in rural areas accounts for 30% of gov spending on health, whilst rural ares get 70%, yet only 20% live in urban areas...
(Page 15) Adding on from the report it stated:
- lack of supplies caused poor quality of care
- 10% of healthcare spending was on treatment of HIV
- utilization of facilities is low and this is due to a high cost of healthcare. Healthcare is not always free on point of delivery in Kenya.
The document summarizes and gives the following suggestions:
- focus should be on improving the human capacity. Ie. more training and hiring, health workers and agricultural extension officers
- 39% should go to operations and maintenance. ie. on provision of anti malaria drugs and mosquto nets
- 19% should go towards investment in infrastructure
- In medium term spending should be focused on adding human capital and improving infrastructure especially down trunk road.